

How Voice AI Breaks Language Barriers in Pharma

Key Takeaways
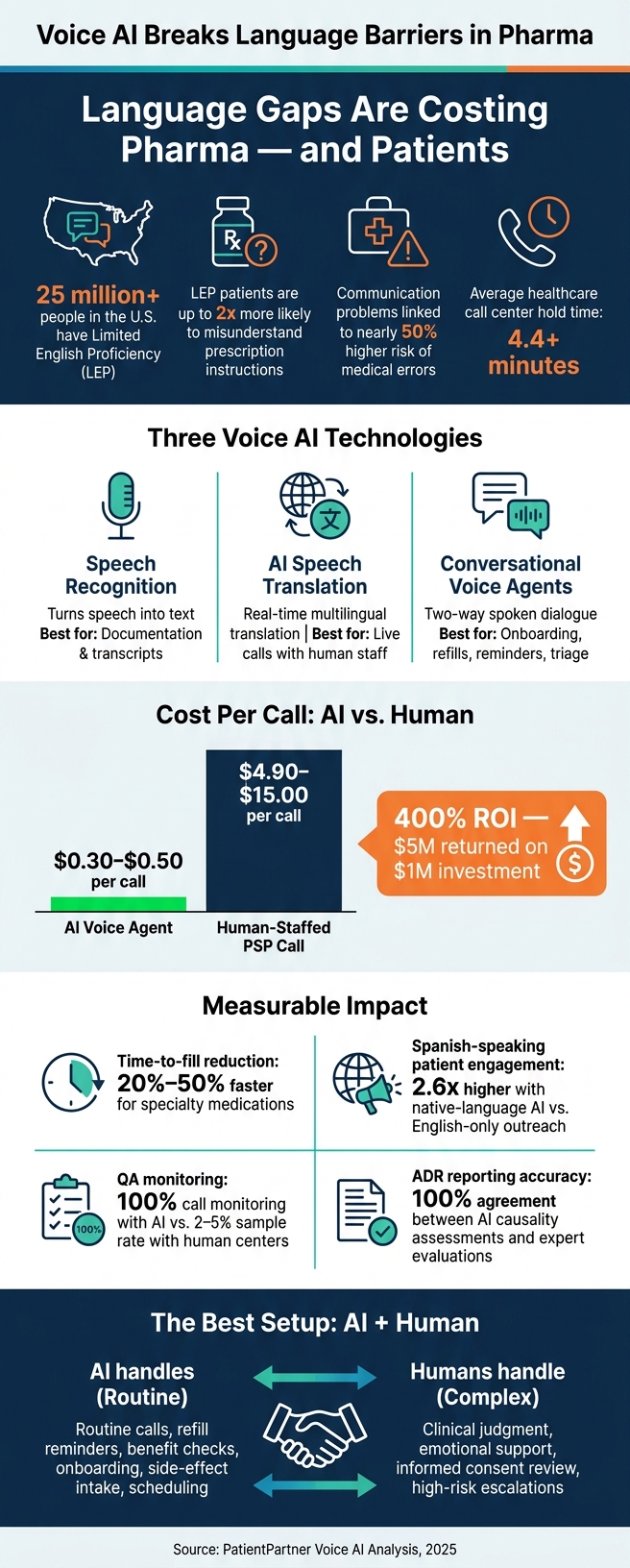
Voice AI can help pharma teams cut language gaps, shorten wait times, and keep more patients on therapy. In the U.S., more than 25 million people have limited English proficiency, and many support programs still start in English. That gap can slow onboarding, delay first fills, and hurt adherence.
Here’s the short version:
- I see three main voice AI tools in this space: speech recognition, live translation, and conversational voice agents
- I’d use them in different parts of the patient journey, from onboarding and refill reminders to trial support and side-effect intake
- The biggest gains tend to show up in access, call handling, and follow-through
- The main guardrails are HIPAA-safe data handling, script control, testing by language and accent, and human escalation for high-risk cases
- The best setup is usually AI for routine calls, people for clinical judgment and emotional support
A few numbers explain why this matters:
- LEP patients can be up to 2x more likely to misunderstand prescription instructions
- Communication problems are tied to a nearly 50% higher risk of medical errors
- Average healthcare call center hold times can run past 4.4 minutes
- AI voice agents may cost about $0.30 to $0.50 per call, versus $4.90 to $15.00 for human-staffed PSP calls
- One case cited a 400% ROI, with $5 million returned on a $1 million investment
If I were reading this article for one takeaway, it would be this: voice AI is less about replacing people and more about making multilingual support available the moment a patient needs help.
| Tool | What it does | Best fit |
|---|---|---|
| Speech recognition | Turns speech into text | Documentation and transcripts |
| Live translation | Translates speech during a call | Multilingual conversations with human staff |
| Conversational voice agents | Handles two-way spoken tasks | Onboarding, refills, reminders, triage |
So the core question is simple: where should AI speak for your team, and where should a person step in?
Voice AI vs. Human Support in Pharma: Cost, Scale & Impact
How voice AI removes language barriers across the patient journey
Multilingual onboarding, education, and adherence support
The biggest wins show up after enrollment. That’s when patients still need clear instructions, refill reminders, and follow-up in the language they’re most comfortable with.
Voice AI can guide onboarding, walk patients through treatment steps, and keep support in their preferred language. Newer systems can detect a patient’s language and keep the conversation going without starting over. They can also hold context even if the patient switches languages mid-call. Natural language processing helps turn medical jargon into plain English, or plain Spanish, Mandarin, Arabic, and so on. That matters when you’re explaining dosing, side effects, and what patients need to do next.
Automated outreach can take care of refill reminders and dose confirmations. If a patient misses several doses or reports a side effect, the system can route the case to a staff member on its own.
Clinical trial communication and side-effect reporting
In clinical trials, voice AI can help with recruitment, informed consent, and side-effect reporting for patients with limited English proficiency. If a patient has trouble describing symptoms or doesn’t fully understand consent language, voice AI can step in with scripted consent prompts that include required safety disclosures. Workflow controls make sure those disclosures are never skipped.
Side-effect reporting is one area where the accuracy jump stands out. A September 2025 study at Mahatma Gandhi Memorial Medical College looked at an AI-enabled adverse drug reaction (ADR) reporting system across 100 participants. The system delivered very high transcription and translation accuracy. Its AI-generated causality assessments showed 100% agreement with expert evaluations, showing that AI can process and sort side-effect reports with a high level of accuracy.
When patients can report issues in their own language, at any hour, pharmacovigilance teams get faster and more complete data.
That same dependability matters when voice AI is used for day-to-day support, not just trial workflows.
Call center automation without losing patient clarity
AI voice agents can handle refills, benefit checks, and scheduling while cutting wait times. In one 2025 deployment for a major pharmaceutical company, voice agents handled benefit checks and delivered a 400% ROI - a $5 million return on a $1 million investment - while bringing verification turnaround down to under 6 hours.
When a call needs a person, the AI can pass along the detected language, reason for escalation, and full conversation context so the patient doesn’t have to repeat everything. Some systems also give the human agent a real-time English transcript while the patient keeps speaking in their native language.
The most important function changes based on the job at hand: transcription, translation, or full conversation.
sbb-itb-8f61039
Voice AI technologies pharma teams are evaluating
Pharma teams tend to look at three main options: speech recognition, real-time translation, and conversational voice agents. Each one fits a different job. Some are best for documentation. Others help with live translation. And some are built for direct patient conversations.
Speech recognition vs. translation vs. conversational agents
| Technology Type | Core Function | Typical Pharma Use Case | Strengths | Key Limitations |
|---|---|---|---|---|
| Speech Recognition (ASR) | Transcribes spoken language to text | Medical documentation; conference transcription | Fast; accurate for technical terms | No translation or interactive capability |
| AI Speech Translation | Translates speech in real time | Global investigator meetings; clinical consultations | Breaks language barriers; supports multilingual communication | Accuracy varies by dialect and speech quality |
| Conversational Voice Agents | Interactive, multi-turn dialogue with context retention | Patient support programs; benefit verification; adherence follow-up; appointment scheduling; prescription refills | 24/7 availability; strong script adherence; scalable; reduces staff workload | Requires careful configuration |
The choice comes down to what the team needs the system to do.
- Speech recognition is mainly for turning spoken words into text. That makes it useful for medical documentation and conference transcription, but it doesn't translate speech or carry on a back-and-forth exchange.
- AI speech translation is built for live multilingual communication, like global investigator meetings or clinical consultations. It can help teams bridge language gaps, though results can shift based on dialect and audio quality.
- Conversational voice agents are meant for multi-step patient interactions. Think patient support programs, benefit verification, adherence follow-up, appointment scheduling, and prescription refills. They can stay available 24/7, follow scripts closely, and handle large call volume without adding staff, but setup needs care.
Cost is one of the biggest reasons teams pay close attention to voice agents. AI agents run at about $0.30 to $0.50 per call, while human-staffed PSP calls usually land between $4.90 and $15.00 per call. When call volume climbs, that spread adds up fast.
Where PatientPartner can add value alongside voice AI
PatientPartner can step in when automation isn't enough. If a patient needs reassurance, lived-experience guidance, or a more personal handoff after automated outreach, human mentorship can fill that gap.
So even after a team picks the right category, the work isn't done. They still need HIPAA-ready workflows, accurate handling, and clear ways to track results. Then comes the next checkpoint: whether the platform fits U.S. privacy, accuracy, and workflow demands.
Compliance, implementation, and measurement in the U.S.
Once the use case is clear, the next hurdle is simple: can the workflow stay HIPAA-safe, stay accurate, and prove its value?
HIPAA, data handling, and accuracy requirements
Treat voice data as sensitive biometric PII. That means requiring BAAs across telephony, transcription, model, and TTS vendors, using TLS 1.2+ for data in transit, AES-256 for data at rest, and running automated PII redaction before anything is stored or passed downstream.
Accuracy needs firm standards too. Set clear transcription and translation thresholds, then test them against accents, dialects, and noisy audio before launch. If a system performs well in a clean demo but falls apart on a busy clinic line, that's a problem waiting to happen.
For routine flows, machine translation is often enough. But informed consent, treatment plans, and eligibility decisions should go to a qualified human translator or live interpreter. In plain English: use AI where the task is routine, and bring in people where the stakes are high.
Three controls matter most here:
- Infrastructure-level redaction
- Policy-level script enforcement
- Automatic escalation for adverse events or distress
That setup helps teams limit risk without slowing every interaction to a crawl.
How to measure value beyond call volume
Measure the workflows voice AI actually touches, like onboarding, refills, trial reporting, and escalations.
Call volume is just a proxy. It tells you activity, not results. The numbers that matter to commercial, patient experience, and compliance teams vary by function.
For commercial teams, the key metrics are time-to-fill for specialty medications, first-fill rates, and long-term refill persistence. Voice AI can cut time-to-fill by 20% to 50%.
For patient experience teams, language-specific engagement is where things get interesting. Spanish-speaking patients showed 2.6x higher engagement when contacted by native-language AI agents instead of English-only outreach.
Compliance teams get something human-staffed call centers usually can't offer at scale: 100% call monitoring with full audit trails, versus the 2% to 5% QA sample rate common in human-run centers. Immutable logs should record language preference, the modality used (AI vs. human), and interpreter IDs for every interaction.
Implementation trade-offs across common pharma use cases
The best deployment model depends on the job. Patient support programs, clinical trial tools, and call center automation may all use voice AI, but they don't play by the same rules. Each one comes with its own compliance demands, integration work, and success metrics.
| Use Case | Primary Benefit | Compliance Considerations | Integration Needs | Success Metrics |
|---|---|---|---|---|
| Patient Support Assistant | Adherence and refill support | BAA required; adverse event queries must escalate to human agents | EHR (Epic/Cerner) & CRM (Salesforce) | Refill persistence; first-fill rate; adherence % |
| Clinical Trial Translation | Faster recruitment of diverse populations | Validated patient-reported outcome translations; informed consent forms require human review | Clinical Trial Management System (CTMS) | Enrollment diversity; participant retention; BLEU scores |
| Multilingual Call Automation | Routine inquiry automation | Verbatim script enforcement; PII redaction; full audit trails | Telephony (SIP/PBX) & helpdesk (Zendesk) | Call abandonment rate; resolution speed; cost per interaction |
One practical move helps across all three: keep translatable scripts separate from PHI so teams can update languages without exposing patient data.
The most workable setup is usually hybrid. AI handles routine interactions, while humans step in for clinical judgment and emotional support.
Conclusion: What pharma leaders should take away
Language barriers still slow access, understanding, and adherence across U.S. pharma. Voice AI is one of the most practical tools on the table for closing that gap at scale.
The main move is simple: AI should take routine, high-volume interactions, while people should step in for clinical edge cases and emotional moments. That split may look a little different by team, but the model stays the same.
Key points for commercial, patient experience, and compliance teams
Commercial teams should put native-language engagement first and tie it to measurable ROI.
Patient experience teams should focus on access between clinical touchpoints. Voice AI gives patients 24/7 multilingual access across many languages. PatientPartner can add a human layer when someone needs reassurance, guidance, or a personal handoff.
Compliance and regulatory teams should focus on auditability, script control, and automatic escalation, with approved scripts and guardrails built into the workflow.
Across teams, the pattern is clear: automate routine work, escalate exceptions, and keep tight control over the workflow.
Voice AI works best when operations, governance, and workflow design are set before launch.
FAQs
When should a human take over from voice AI?
Human intervention matters most when a conversation turns sensitive or emotional, like sharing hard news or helping a patient who is clearly distressed.
Staff should also step in if background noise interferes with the technology or if the system doesn't have the expert knowledge needed for safety and accuracy. In more complex healthcare conversations, bringing in a person helps protect patient trust.
How do pharma teams test voice AI across languages and accents?
Pharma teams test voice AI to make sure it gets both the technical language and the spoken language right across many speech patterns. These systems usually combine speech recognition, natural language processing, and text-to-speech, with training built around medical terms.
The target is usually at least 90% word accuracy across accents and regional dialects. To check that, teams run pilot programs and compare the system’s performance against human baselines. They also look at error reduction, how well the system switches languages, and whether it keeps the right context during multilingual conversations.
What should companies measure first after launch?
After launch, companies should first measure production-grade deployment evidence - not just pilot results or watered-down metrics.
That means looking at what happens in live use: actual call volumes, self-service resolution rates for routine tasks, and offload rates that hold up for at least 12 months. It also means tracking patient experience scores and health equity outcomes.
In plain English, the goal is simple: measure what works in the messiness of day-to-day care, not just what looked good in a short test.
Related Blog Posts
Author

